
Bariatric surgery significantly reduces all-cause mortality and death from cardiovascular disease, diabetes, and cancer in patients with severe obesity, according to a 40-year retrospective study published in Obesity. However, the study also found an increased risk of death from chronic liver disease and higher suicide rates among younger post-surgery patients, highlighting the need for comprehensive pre- and post-surgery psychological care.
Younger population experiences increased risk of death from suicide and chronic liver disease.
A new retrospective study with up to 40 years of follow-up shows significant reductions in death rates from all causes and cause-specific conditions such as cardiovascular disease, diabetes and cancer in patients who have undergone bariatric surgery compared to non-surgical participants with severe obesity, according to a new study published in Obesity, The Obesity Society’s (TOS) flagship journal.
The study also found evidence suggesting increased risk of death from chronic liver disease, in addition to higher death rates from suicide in younger patients who had bariatric surgery compared to non-surgical participants. The study’s authors observe that the findings of increased suicide rates among younger patients who have had bariatric surgery may promote more aggressive, pre-surgical psychological screening and post-surgery follow-up.
As a result of the decades-long durability of bariatric surgery in reducing death from all causes and decreasing deaths related to cardiovascular disease, diabetes, and cancer compared to matched participants, researchers note the findings may not only increase interest in bariatric surgery treatment for patients with severe obesity but, in addition, further stimulate important research related to the discovery of physiologic and biomolecular mechanisms leading to non-surgical treatment that results in weight loss and improved mortality similar to that achieved by bariatric surgery, said Ted D. Adams, Intermountain Surgical Specialties/Digestive Health Clinical Program, Intermountain Healthcare, Salt Lake City, Utah; Division of Epidemiology, Department of Internal Medicine, School of Medicine and Department of Nutrition and Integrative Physiology, University of Utah, Salt Lake City. Adams is the corresponding author of the study.
Experts explain that multiple association studies connecting bariatric surgery and mortality outcomes have been reported, predominantly retrospective, with wide variation in study design pertaining to participant number, control cohorts, mean follow-up, procedure type, age at surgery, clinical end points such as life expectancy and death rates for all causes and specific causes, and presence or absence of prevalent diabetes. The new study builds upon the groups’ reported mortality outcomes following gastric bypass surgery by extending follow-up to 40 years, tripling the number of surgical patients, and using four, instead of one, bariatric surgery procedures.
Researchers used data from the Utah Population Database (UPDB) for the current study. The UPDB includes linked, population-based information from Utah with statewide birth and death certificates, driver licenses and ID cards, and voter registration cards. The UPDB creates and maintains links between the database and the medical records held by the two, largest healthcare providers in Utah.
Patients who had undergone bariatric surgery in Utah between 1982 and 2018 were identified from three, large bariatric surgical practices in Salt Lake City, Utah, and from medical records from the University of Utah and Intermountain Healthcare Enterprise Data Warehouses in Salt Lake City. Non-surgical participants were selected from Utah driver license records or ID cards. Because driver licenses are generally renewed every five years, multiple records were available for selection for matching to the bariatric surgeries.
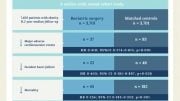
Nearly 22,000 participants with bariatric surgery and without were matched (1:1) for age, sex, body mass index and surgery date with a driver license/renewal date. Mortality rates were compared by Cox regression and stratified by sex, surgery type, and age at surgery. Whereas mortality after gastric bypass surgery was previously reported from 1984 to 2002, this study extends mortality follow-up through 2021. The four bariatric surgery procedures included Roux-en-Y gastric bypass, adjustable gastric banding, sleeve gastrectomy, and bilio-pancreatic diversion with duo-denal switch.
Results revealed that all-cause mortality was 16% lower in patients who had bariatric surgery compared to non-surgical participants. Lower mortality was observed for both males and females. Mortality after surgery versus non-surgery decreased by 29%, 43%, and 72% for cardiovascular disease, cancer and diabetes, respectively. Death rates for males and females from chronic liver disease were 83% higher in patients who had surgery compared to non-surgical participants. The hazard ratio for suicide was 2.4 times higher in surgery compared with non-surgery participants, primarily in individuals with ages at surgery between 18 and 34 years.
“This important study adds to the mounting evidence that bariatric surgery, not only improves quality of life for patients, but will also increase their life expectancy. This work will hopefully improve patients’ access to this effective treatment for obesity, which is still limited to only one percent of qualified patients. Also, the study highlights the importance of providing more resources for pre-surgical psychological screening and post-surgery follow-up, especially for younger patients,” said Jihad Kudsi, MD, MBA, MSF, DABOM, FASMBS, FACS, Bariatric Surgery Division, Duly Health and Care, Downers Grove, Ill. Kudsi was not associated with the research.
Reference: “Long-term All-Cause and Cause-Specific Mortality for Four Bariatric Surgery Procedures” by Ted D. Adams, Huong Meeks, Alison Fraser, Lance E. Davidson, John Holmen, Michael Newman, Anna R. Ibele, Nathan Richards, Steven C. Hunt and Jaewhan Kim, 25 January 2023, Obesity.
DOI: 10.1002/oby.23646
Other study authors include Nathan Richards, Intermountain Surgical Specialties/Digestive Health Clinical Program, Intermountain Healthcare, Salt Lake City, Utah; Lance E. Davidson and Steven C. Hunt, Division of Epidemiology, Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City. Davidson is also with the Department of Exercise Sciences, Brigham Young University, Provo, Utah. Hunt is also associated with Department of Genetic Medicine, Weill Cornell Medicine, Doha, Qatar. Huong Meeks and Alison Fraser, Huntsman Cancer Institute, University of Utah; John Holmen, Intermountain Biorepository, Intermountain Healthcare, Salt Lake City; Michael Newman, University of Utah Health, Data Science Services; Ana R. Ibele, Division of General Surgery, Department of Surgery, University of Utah School of Medicine; and Jaewhan Kim, Department of Physical Therapy, College of Health, University of Utah.
Adams has received research funding from National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases (NIH-NIDDK), Ethicon Endo-Surgery (Johnson & Johnson), and Intermountain Medical Research and Education Foundation of Intermountain Healthcare. Davidson has received funding from NIH-NIDDK. Hunt has received funding from NIH-NIDDK and the Biomedical Research Program at Weill Cornell Medicine in Qatar, a program funded by the Qatar Foundation. All other authors declared no conflict of interest.







Bariatric surgery just treats the symptoms not the cause.
I’ve seen it play out in real time with several of my friends.
The weight loss lasts for a few years but as time goes by they return to the same eating habits and gain the weight back.
Food is an addiction and until it’s recognized as such, there will be no change 🙁
We need to change the food industry. Humans need to eat less processed garbage that contains all those chemicals, additives and refined sugar and flour.
Agreed, but follow the money; processed foods = political and corporate power.
We need a CULTURAL change.