
The first doses of the Pfizer Covid-19 vaccine are administered to Iowa State University health care employees on Friday, December 18, 2020, at the Thielen Student Health Center. Credit: Christopher Gannon/Iowa State University
A year ago, amid surging COVID-19 cases and a limited supply of newly developed vaccines, the U.S. Centers for Disease Control and Prevention faced a big question: Who should be at the front of the line to get a vaccine? Students living in college dorms or people living with chronic kidney disease? Grandmas or teachers? Along with goals of reducing overall infections and deaths, the CDC aimed to prevent hospitals from getting overwhelmed and ensure equitable access to COVID-19 vaccines.
Iowa State University researchers were part of a team evaluating 17.5 million possible strategies the CDC could have recommended last winter to state, territorial, tribal and local governments for COVID-19 vaccine rollouts. In a newly published paper, the researchers generally validate the CDC’s ultimate recommendation, while the mathematical model the team developed also highlights some minor improvements. The work could help inform the design of future vaccination strategies in the U.S. and abroad.
The CDC recommended four staggered priority groups for COVID-19 vaccines:
- Phase 1a included health care personnel and residents of long-term care facilities.
- Phase 1b included non-health care frontline essential workers (e.g. police officers, firefighters, child care workers) and people 75 and older.
- Phase 1c included other essential workers (e.g. bus drivers, bank tellers), 16-64 year-olds with increased risk of severe COVID-19 disease and 65-74 year-olds.
- Phase 2 included 16-64 year-olds without high risk conditions or comorbidities.
“The CDC strategy did really well when we compared it to all the other possible strategies, especially in preventing deaths across age groups,” said Claus Kadelka, an assistant professor of mathematics and the corresponding author of the paper published in PLOS ONE. “Our research shows the CDC’s higher prioritization of frontline essential workers, people in older age groups and people with underlying health factors was a highly effective strategy for curbing COVID-19 mortality, while keeping overall case numbers at bay.”
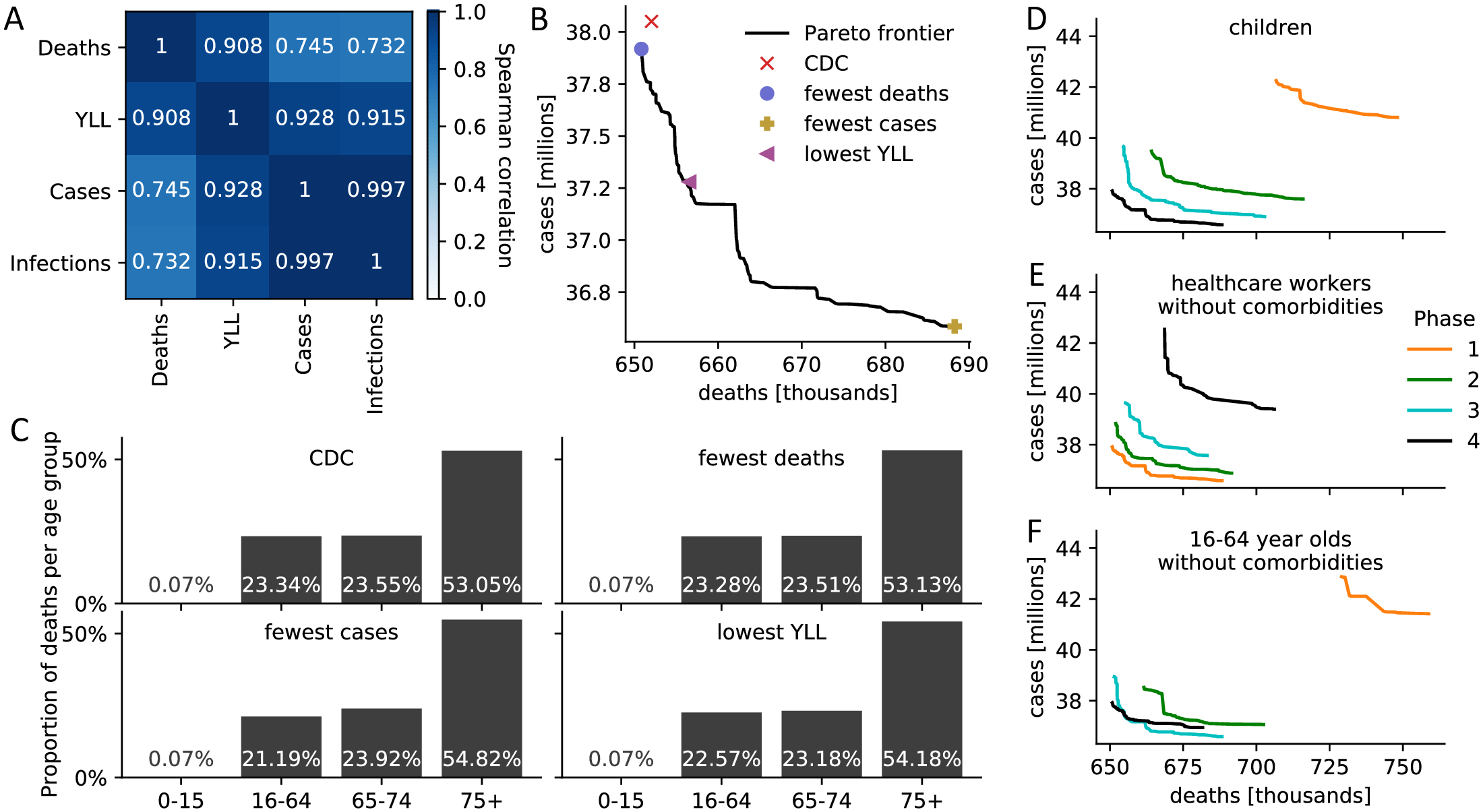
(A) Spearman correlation between four measures of disease burden based on a complete comparison of all 17.5 million meaningful four-phase vaccine allocation strategies. (B) Pareto frontier of all optimal strategies based on a global search of all 17.5 million meaningful vaccine allocation strategies. For strategies on the Pareto frontier, there exists no other strategy that performs better in one objective (minimizing deaths or cases) while not performing worse in the other objective. The death and case count resulting from four specific allocations is highlighted. (C) For the four strategies highlighted in (B), the distribution of all resulting deaths across the four age groups is shown as a measure of equity. (D-F) Pareto frontiers of all optimal strategies are shown when restricting (D) children, (E) healthcare workers without comorbidities, (F) 16–64 year old without comorbidities and without an essential occupation to a certain priority phase. S8 Fig contains Pareto frontiers for all sub-populations. Credit: Islam et al., 2021, PLOS ONE, CC-BY 4.0
To evaluate the CDC’s recommendations, Kadelka and the research team built a mathematical model that incorporated the agency’s four staggered phases for a vaccine rollout and 17 sub-populations based on factors like age, living conditions and occupation. Individuals fell into one of 20 categories, such as “susceptible to the virus,” “fully vaccinated,” “currently infected,” “infected but without COVID-19 symptoms” and “recovered.” The researchers also incorporated several important characteristics of the COVID-19 pandemic, such as vaccine hesitancy, social distancing levels based on current caseloads in the U.S. and different infection rates for different virus variants.
“We ran the model 17.5 million times on the ISU supercomputer, and for each run, we recorded and finally compared several outcome metrics: predicted number of deaths, predicted number of cases, and so on,” Kadelka said.
Vaccinating children in any but the last phase of the vaccine rollout always led to a non-optimal outcome in the model. The researchers said the CDC’s recommendations could have been optimal if more individuals with known COVID-19 risk factors had been prioritized over people in their cohort without health risks. However, the gains would have been small (i.e. less than 1% fewer deaths and overall years of life lost, and 4% fewer cases and infections), and Kadelka said the model does not take into account possible logistical challenges.
“We don’t know enough about the situation in nursing homes to know how easy it would be to distinguish which residents have greater risk factors that would put them at the front of the vaccination line. That’s something you can do in a mathematical model, but it could be hard in practice,” Kadelka added.
Kadelka said part of what makes the model unique is that it takes into account the extent to which a vaccine prevents someone from getting infected, developing symptoms and passing the virus on to others, all of which can change over time, or even vary depending on the particular vaccine. The researchers show that the ideal vaccination strategy is sensitive to these parameters, which are still mainly unknown.
Md Rafiul Islam, a postdoc in Kadelka’s group and the lead author of the paper, said the mathematical model could help inform the design of current and future vaccination strategies.
“Our model is useful to identify an optimal vaccine allocation strategy and can be easily expanded to answer questions related to booster allocation in the face of waning immunity and increasing virus variability,” Islam said.
Kadelka added, “If the (SARS-CoV-2) virus mutated enough that it rendered the current vaccines ineffective or we have a new pandemic, whether that’s in another 100 years or two years from now, we need to be able to accurately predict what the outcome will be when decisions are made regarding who’s vaccinated first.”
Developing a vaccine strategy is complicated, and there will always be tradeoffs between opposing goals like minimizing mortality or incidence. But Kadelka believes mathematical models like the one he and his colleagues created can help ensure lifesaving vaccines can have the greatest impact.
Reference: “Evaluation of the United States COVID-19 vaccine allocation strategy” by Md Rafiul Islam, Tamer Oraby, Audrey McCombs, Mohammad Mihrab Chowdhury, Mohammad Al-Mamun, Michael G. Tyshenko and Claus Kadelka, 17 November 2021, PLoS ONE.
DOI: 10.1371/journal.pone.0259700







Be the first to comment on "Did the CDC’s COVID-19 Vaccine Strategy Work? Comparing 17.5 Million Options"