
The problem with opioids is that they kill pain – and people. In the past three years, more than 125,000 persons died from an opioid overdose – an average of 115 people per day – exceeding the number killed in car accidents and from gunshots during the same period.
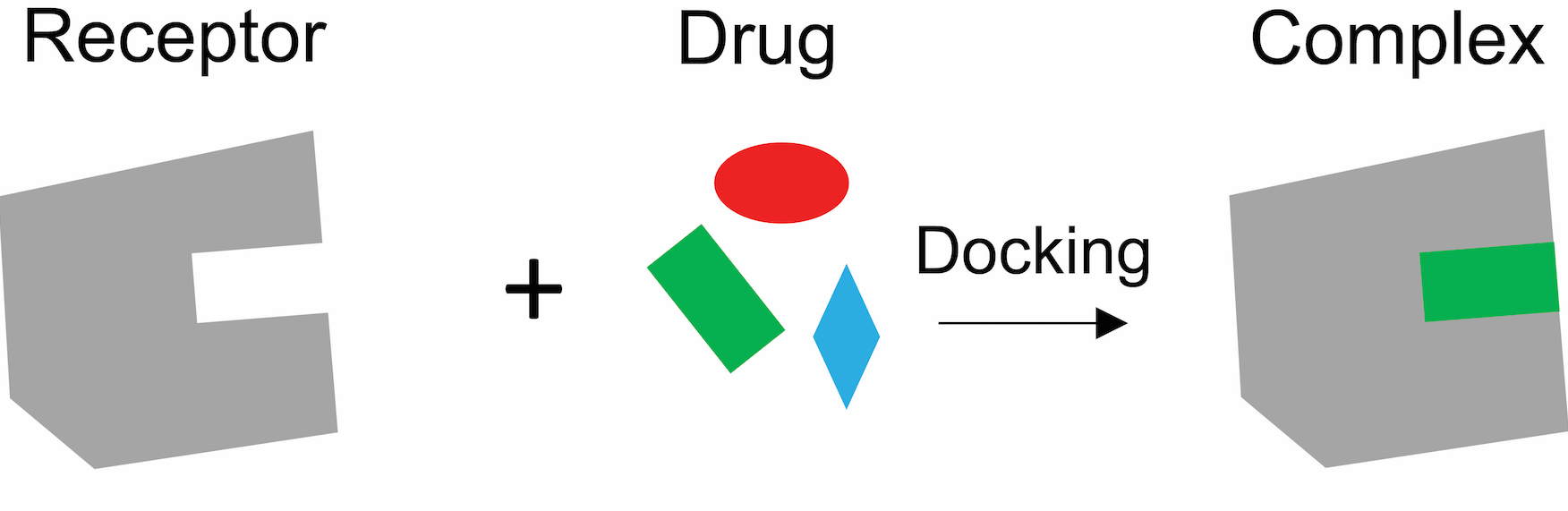
America desperately needs safer analgesics. To create them, biochemists like myself are focusing not just on the opioids, but on opioid receptors. The opioids “dock” with these receptors in the brain and peripheral nervous system dulling pain but also causing deadly side effects.
My colleagues and I in Bryan Roth’s lab have recently solved the atomic structure of a morphine-like drug interacting with an opioid receptor, and now we are using this atomic snapshot to design new drugs that block pain but without the euphoria that leads to addiction.
What has caused the opioid epidemic?
In the U.S., more than one-third of the population experiences some form of acute or chronic pain; in older adults, this number rises to 40 percent. The most common condition linked to chronic pain is chronic depression, which is a major cause of suicide.
To relieve severe pain, people go to their physician for powerful prescription painkillers, opioid drugs such as morphine, oxycodone and hydrocodone. Almost all the currently marketed opioid drugs exert their analgesic effects through a protein called the “mu opioid receptor” (MOR).
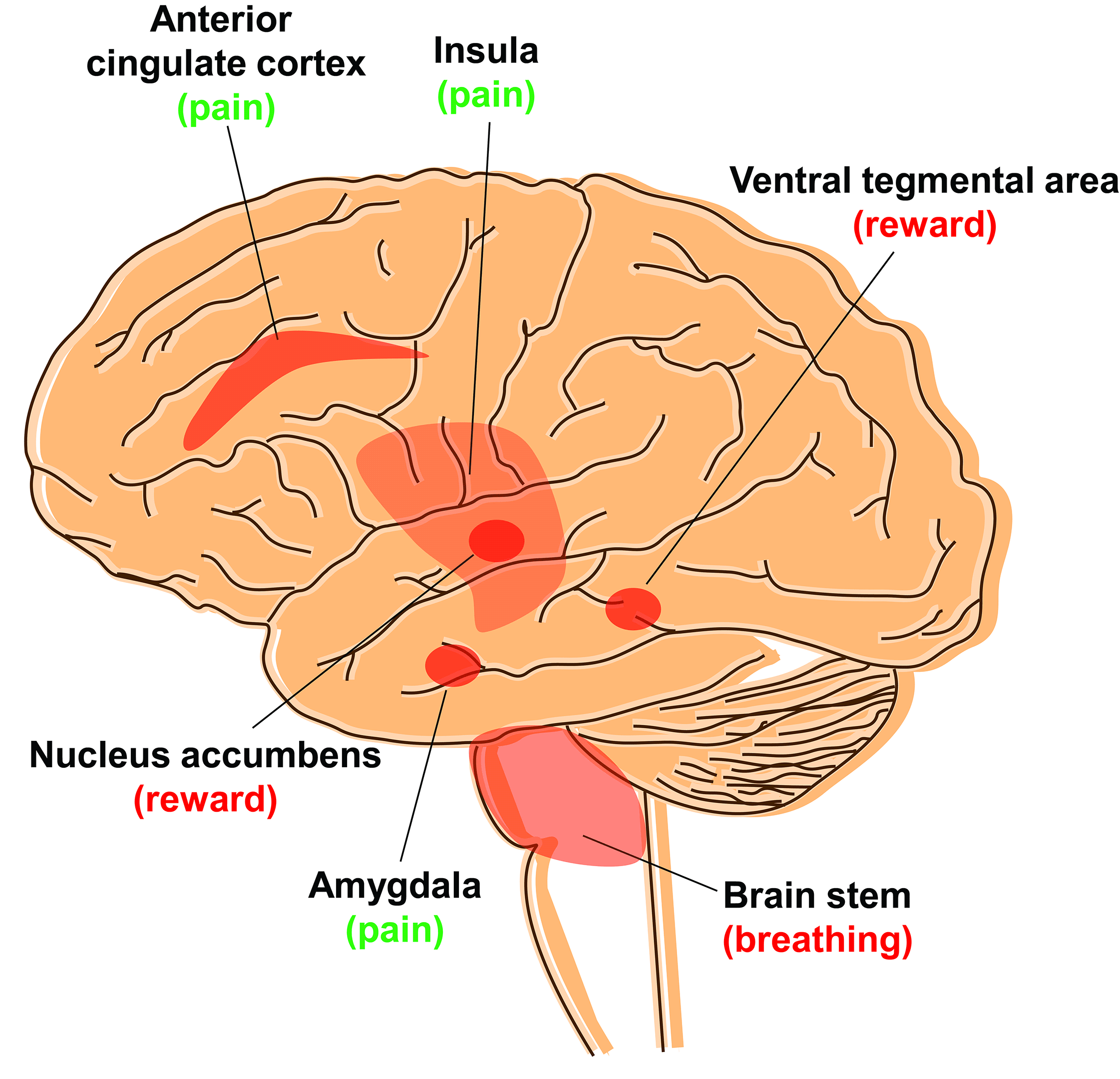
MORs are embedded in the surface membrane of brain cells, or neurons, and block pain signals when activated by a drug. However, many of the current opioids stimulate portions of the brain that lead to additional sensations of “rewarding” pleasure, or disrupt certain physiological activities. The former may lead to addiction, or the latter, death.
Which part of the brain is activated plays a vital role in controlling pain. For example, MORs are also present in the brain stem, a region that controls breathing. Activating these mu receptors, not only dulls pain but also slows breathing. Large doses stop breathing, causing death. Activating MORs in other parts of the brain, including the ventral tegmental area and the nucleus accumbens, block pain and trigger pleasure or reward, which makes them addictive. But so far there is no efficient way to turn these receptors “on” and “off” in specific areas.
But there is another approach because not all opioids are created equal. Some, such as morphine, bind to the receptor and activate two signaling pathways: one mediating pain cessation and the other producing side effects like respiratory depression. Other drugs favor one pathway more than the other, like only blocking pain – this is the one we want.
“Biased opioids” to kill pain
But MOR isn’t the only opioid receptor. There are two other closely related proteins called kappa and delta, or KOR and DOR respectively, that also alter pain perception but in slightly different ways. Yet, currently there are only a few opioid medications that target KOR, and none that target DOR. One reason is that the function of these receptors in the brain neurons remains unclear.
Recently KOR has been getting attention as extensive studies from different academic labs show that it blocks pain without triggering euphoria, which means it isn’t addictive. Another benefit is that it doesn’t slow respiration, which means that it isn’t lethal. But although it isn’t as dangerous as MOR, activating KOR does promote dysphoria, or unease, and sleepiness.
This work suggests it is possible to design a drug that only targets the pain pathway, without side effects. These kind of drugs are called “biased” opioids.
Discovering and designing drugs to target KOR
So far, there are two popular ways to discover new drugs. The first involves using existing commercially available libraries of compounds and testing them on cells or animals to find one that has the required characteristics. This hit-and-miss approach is straightforward but time-consuming, running anywhere from three months to two years to screen between 3,000 to 20,000 compounds.
The other strategy is called “structure-based drug design.” With this approach, you first need a high-resolution photograph of the receptor – showing the arrangement of every atom in the molecule. Then, using a computer program, you can examine up to 35 million molecules from a virtual chemical library called ZINC 15 to find a molecule that will precisely interact – lock-and-key style – with the receptor. It is like having the precise dimensions of the International Space Station so that you can design a spacecraft that can fits perfectly in the docking site.
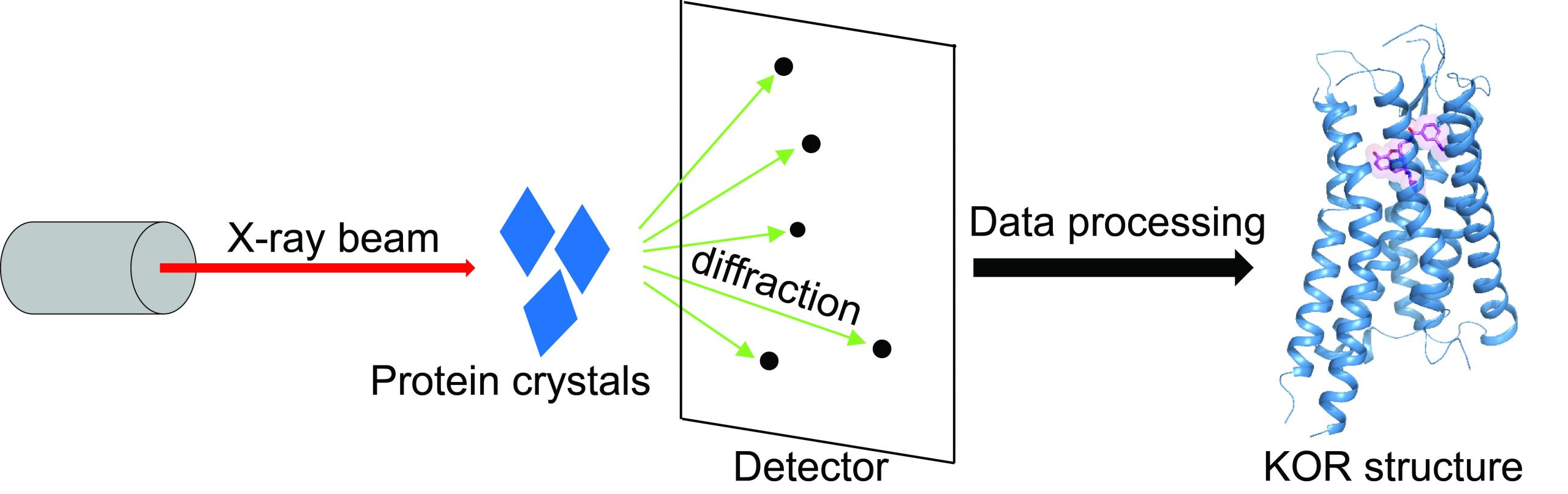
I’m a crystallographer, which means I specialize in taking atomic resolution photographs of proteins. I became interested in solving the structure of KOR – when the protein is in its active state bound to a drug.
Structure is considered the gold standard for figuring out how a drug interacts with a receptor and produces a signal. To solve the KOR structure, I first manufactured the KOR protein to make KOR crystals, which consists of hundreds of millions of KOR molecules stacked in the same way, just like salt molecules in a salt crystal. Then I blasted the crystals with X-rays to generate an image of the receptor at atomic level. The key to these pictures was that I “froze” the KOR proteins in their active state to understand how these receptors interact with a drug.
With an action shot of KOR, we recognized what parts of the molecule are critical for blocking pain signals. We are now using this structural data to construct a “biased” molecule that only activates the pain-blocking parts of the protein without triggering side effects.
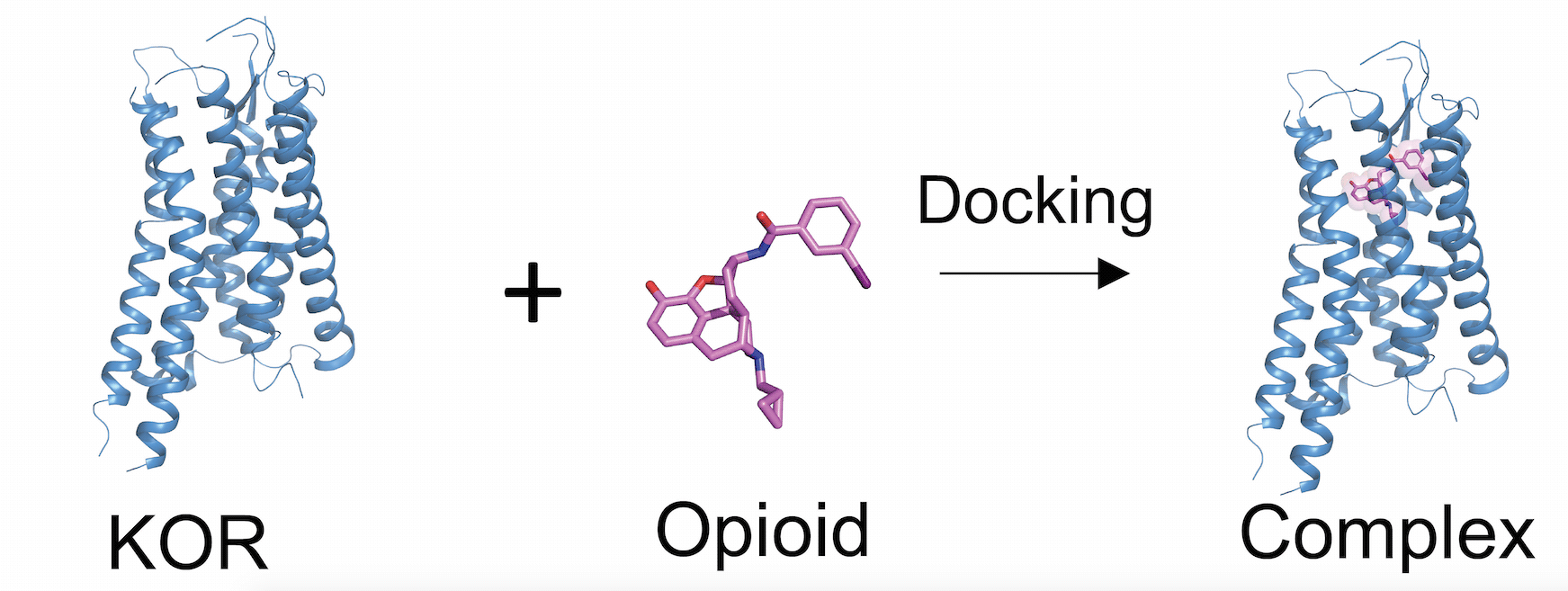
Deciphering the structure of a protein is also valuable for creating a drug that interacts with only one receptor. All the members of the opioid receptor family – MOR, KOR, and DOR – look similar, like siblings. Therefore, these high-resolution photos are essential for designing drugs that will only recognize and target KOR.
Our structure is now used for virtual drug screening where the computational program randomly inserts millions of compounds into the structure and ranks each of them based on how well they fit. The better the score, the more likely that compound will yield a drug.
The exciting news is that researchers in the Roth lab have discovered several promising compounds based on the KOR structure that selectively bind and activate KOR, without cavorting with the more than 330 other related protein receptors.
Written by Tao Che, Postdoctoral Research Associate at Department of Pharmacology, University of North Carolina at Chapel Hill.
This article was first published in The Conversation.![]()
Never miss a breakthrough: Join the SciTechDaily newsletter.
Follow us on Google and Google News.
13 Comments
For decade a popular anti-diarrhea medicine (available in Mexico) is made of opium and an amphetamine. Works great with no side effects. Preferred by pilots.
Rx Opioids are safe/effective when used as directed. The #’s you have in the first paragraph of this article are incorrect. You didn’t happen to mention the fact that the opioids were not even theirs in the post mortems & that most of them are Illicit opioids (fentanyl analogus, heroin) and Mixtures of amphetamines, alcohol with an opiate and something else. That needed to be pointed out because the propaganda is indirectly killing pain Patients that take their med correctly. I do see what you’re trying to do here, but let me ask you this. what is wrong with out affordable, tried and true medications?
This article is way off base. Opioids pain killers are safe, effective, and literally do not trigger pleasure when used the way they are intended. The ONLY other medication for pain is tylenol. Pain patients are being tortured by opioid hysteria going after legitimate pain patients and doctors instead of illicit drugs. The two are not the same. Very irresponsible article!
And 53 million Americans suffer in extreme chronic pain because 141,00 Americans choose to abuse drugs.
Totally ludicrous. Who is representing Americans, truly?
Was this paid for by the Sacklers?
Hoe Many People Die from Reasons Related To Alcohol Every year ?
And How Many of those Are Deaths of the innocents At the hands of The Alcoholic !
Let’s Worry about That As Those numbers are Astronomical!!!
One problem with activating kappa receptors is the extreme dysphoria and complete lack of tolerance to cold and hot. If anything we should be trying to come up with kappa antagonists.
I have been on zomorph slow release morphine and oramorph morphine sulphate liquid for chronic pain both knees and one ankle and due to my gp causation not doing mri when I sprained my ankle in May 2019 I have been bedridden 24/7 for 4 years unreal I played football till I was 50 I’m now 58 our gps in UK are more concerned about having opiate addicts than helping people in chronic pain I also have addisons. I’m at the point of stop taking my steroids outcome I’d fatal or taking a garden shredder to remove both legs. As for euphoria what a load of rubbish ..not once in my 5i years have I experienced euphoria except the birth of my two children.there are things out there to help please use your Hypocratic Oath and stop the suffering instead of providing funds for people who are addicts and treat the people who need help
My body has been hacked and slashed in the name of American back surgery (5 of them). Still in horrific pain and cut back on pain meds for years because I may become addicted. All I have to show for it is large bills, seizures and less pain meds. What is the sense…
I’m 58 and have addisons and opiates as my consultant doesn’t like to use ligothaine infusions if work opiates can be stopped.i have never met 1 person who is or has been addicted to opiates ever. Just the people who come into the pharmacy and don’t queue to get their methadone our chronic pain is not self inflicted so get out your BMJ and look at research an alternative to opiates if not don’t assume we are addicts it’s a disgrace we have to suffer in pain whilst the people doing the research don’t have the pain
The only opioid I was getting addicted too was the ones with Tylenol in it. I take Oxycodone with no Tylenol and I have not got that high you get with the big white round pill with Tylenol. I take two 5 mg tablets 3 times a day for my pain without the Tylenol. I don’t know why Dr’s don’t believe me when I say it’s the ones with the Tylenol that get you high not the ones without the Tylenol. I don’t know why people on the street want the ones I take because they are not addictive to me. So they are obviously using it to put with another drug on the street to get high with it That is all I can think of. Because I am now 54 years old and don’t have a clue what these people are doing to get high with it. Things change so fast in the drug world that I can’t imagine what they are doing with the ones I take before me and a girlfriend of mine don’t get high on just oxycodone. It was the big white pill with Tylenol that was getting us high and addicted and I don’t like being addicts to anything because I’m already addicted to cigarettes. I am getting to old for that high business. So I am really curious to know what people do with the kind I take. Because I don’t get high on the ones without Tylenol. I don’t snort them I don’t abuse them at all and I’m the one having to get piss tested all the time because of the drug addicts and it really makes me mad to be treated like that at a pain clinic. They finally are giving us a break on that Everytime we go in. But we still have to count them everything else. So the makers of the ones with Tylenol are the ones getting people addicted and then it stops getting them high so they turn to meth or heroin. I don’t know but I really believe they should take those off the market with the Tylenol. I don’t wish meth on anyone’s family’s. I went through it with my daughter. I let her hit rock bottom let her do her thing but I m not helping her addiction. Either I was gonna wake up and here she’s dead or she was gonna get sick of living on the street and come home to take care of her child . Well I am happy to say she is now clean has got her life together and got rid of all those people in her life and has her daughter back and I got my daughter back . Thanks to God and all her hard work. I know she is very strong because a lot of them don’t come back. It is a very sad addition and hurts the whole family. I love and support her in life for what she has come back from. Let God be with everyone going through this horrible drug. I feel blessed I have her back.
Oh and I don’t always take that many . I was doing pool therapy because the Dr. I was seeing kept doing things to my back that I did not know really what he was doing but he took and kept doing surgery on my back every time I went to see him and the he got mad at me because my insurance would not pay him and I know it was because he was doing things to my back over and over . He said I had the worst insurance ever wel I think he did not get paid because he was doing stuff to my back that he was not supposed to be doing all the time and I’m in worse pain now after he did that and I obviously stopped seeing him. I go to a new pain clinic and they don’t do what he did to me . I was doing pool therapy a long time before Corona hit. I do recommend pool therapy. I felt a lot better doing pool therapy everyday. .But now it’s hard to find a pool with only one life guard and the times of the pool but I guess there is a therapy place I can go to that has a pool so it should be warmer then the YMCA because of my arthritis too and neuropathy and fibromyalgia. But after that I hope I can find a pool that stays open and is not so cold. The warm pool they kick you out every time there is a life guard meeting. Because I also have a hard time leaving my house and I want to go when I feel I can go. But I only take my pills as needed so I do have pills left over when they count them because if I do have to have something else happen to me where I need surgery or a different pain it’s because I’m on oxycodone and another pain trumps my back pain that feels 20 times worse because I’m already on pain pills. So I need to get it under control by exercising in the pool. So keep a eye out on some of these pain Dr.s He would make me say what he was doing before surgery with his boss there so I would try and pronounce what they were doing to me that day and I did not understand what it meant. I just trusted him and I should have not.
I have been taking a Hydrocodone -Acetamin 10-325 Mg tablet twice a day, for chronic back and hip pain, since 2010. I have never once felt any sort of euphoria after taking this medicine. But it has helped with the pain. I have never understood the idea people are getting high and addicted to this product. I had morphine after surgery on two occasions and if I felt euphoric, it was because the pain went away for a while. Nothing more. As a consistent alcohol user for many years, I get how alcohol addiction can occur for some, but definitely not all people: I decided one day to stop drinking and have never missed it.