
The CDC’s vaccine prioritization strategy performed well compared to other approaches, though with some room for improvement.
The four-tiered vaccine prioritization strategy implemented by the US Centers for Disease Control and Prevention (CDC), when compared computationally to all possible COVID-19 vaccine roll-out approaches, performed well by many measures but could be improved upon. The results are published this week in a new study in the open-access journal PLOS ONE by Md Rafiul Islam and Claus Kadelka of Iowa State University, US, and colleagues.
Anticipating an initial shortage of vaccines for COVID-19, the US Centers for Disease Control (CDC) developed priority vaccine allocations for specific demographic groups in the population. This prioritization strategy, and its impact on subsequent disease, has been studied in many ways, but generally only compared to a small number of other vaccine roll-out strategies at a time.
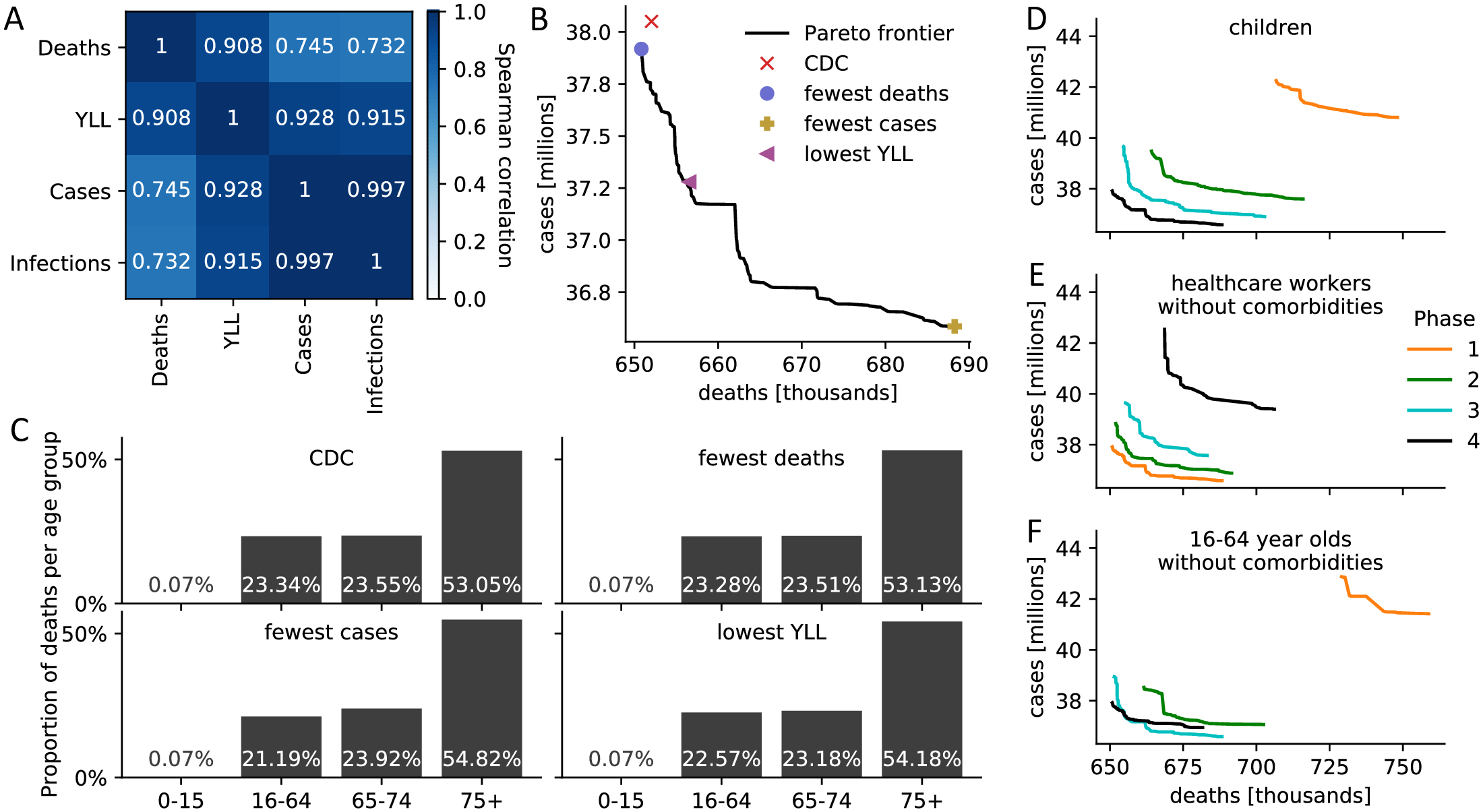
In the new study, Kadelka and colleagues developed a disease model that divided the US population into 17 subpopulations based on the characteristics included in the CDC vaccine recommendation—age, co-morbidity status, job type, and living situation. There are roughly 17.2 billion total ways to allocate vaccines among these 17 subpopulations in up to four phases. The researchers found that only 17.5 million can be optimal. They compared these 17.5 million allocation strategies and analyzed the resulting effect on COVID-19 cases, mortality, and years of life lost (YLL), using well-established assumptions on COVID-19 incubation and spread, vaccine hesitancy, and vaccine effectiveness rates.
According to the analysis, the CDC allocation strategy performed well in all vaccination goals but never ranked the highest of all possible strategies. Compared to the respective optimal methods, the CDC approach led to an estimated 0.19% more deaths, 4.0% more cases, 4.07% more infections and 0.97% higher YLL. Note that there are tradeoffs between the vaccination goals so that no single strategy performs best in objectives: low death counts come, for example, at the expense of higher case counts. The CDC decision to not prioritize the vaccination of individuals under the age of 16 was optimal, as was the prioritization of healthcare workers and other essential workers. However, theoretical strategies which more highly prioritized the vaccination of individuals with comorbidities in all age groups were estimated to improve outcomes. The authors believe that this optimization approach can be used to inform the design of future vaccine allocation strategies around the world.
The authors add: “We developed a model that enables an accurate evaluation of the United States COVID-19 vaccine prioritization. The model further shows how the choice of optimal vaccine strategy depends on parameters such as hesitancy or how a specific vaccine functions.”
For more on this study, read Did the CDC’s COVID-19 Vaccine Strategy Work? Comparing 17.5 Million Options.
Reference: “Evaluation of the United States COVID-19 vaccine allocation strategy” by Md Rafiul Islam, Tamer Oraby, Audrey McCombs, Mohammad Mihrab Chowdhury, Mohammad Al-Mamun, Michael G. Tyshenko and Claus Kadelka, 17 November 2021, PLoS ONE.
DOI: 10.1371/journal.pone.0259700
Never miss a breakthrough: Join the SciTechDaily newsletter.
Follow us on Google and Google News.
1 Comment
The vaccine priority schedule was/is both good and effective, especially considering we’re still in the learning stage of this virus. But the CDC, and all the labs, continue to just focus on the protein spikes to stop the virus from infecting cells in the first place. That’s only half the battle. The virus itself must also be attacked.
All the coronaviruses and all their variants have different protein spikes, with Delta having one that’s more efficient at getting around the vaccines. But the real problem is in the virus itself, not its protein shell, and why the most dangerous (MERS, SARS, and Covid-19) are so infectious. My independent research has found multiple one-in-a-million nucleotide sequence matches between all the coronaviruses and the human genome. Those sequences are the same as some of the loops of human tRNA. Using those loops and their amino acid code matches, viruses may be able to fool the nucleus membrane in cells to allow the virus to enter and associate with the human DNA, creating more opportunities for further infection. Our immune system may be compromised and may no longer be able to stop the virus and other diseases from attacking organs throughout the body. Vaccines that attack the virus protein shells while ignoring their contents are doomed to failure from the Darwin effect, but recognizing these loops suggests a possible approach to successful coronavirus vaccines. Only the infection process is considered in my work, not the innate virulence of the virus. For more info, check out this YouTube, Coronavirus – Using Your DNA Against You. https://www.youtube.com/watch?v=8dOIzD6ch8s