Research reveals that exposure to environmental metals significantly contributes to the buildup of calcium in coronary arteries, similar to traditional risk factors such as smoking and diabetes.
This association offers new insights into the prevention and treatment of atherosclerosis, suggesting that addressing metal exposure could be a crucial step towards reducing cardiovascular disease globally.
Cardiovascular Risks from Metal Exposure
Metal exposure from environmental pollution is associated with increased calcium buildup in the coronary arteries at a level comparable to traditional risk factors like smoking and diabetes, according to a study published today (September 18) in JACC, the flagship journal of the American College of Cardiology. The findings support that metals in the body are associated with the progression of plaque buildup in the arteries and potentially provide a new strategy for managing and preventing atherosclerosis.
“Our findings highlight the importance of considering metal exposure as a significant risk factor for atherosclerosis and CVD,” said Katlyn E. McGraw, PhD, a postdoctoral research scientist at Columbia University Mailman School of Public Health and lead author of the study. “This could lead to new prevention and treatment strategies that target metal exposure.”
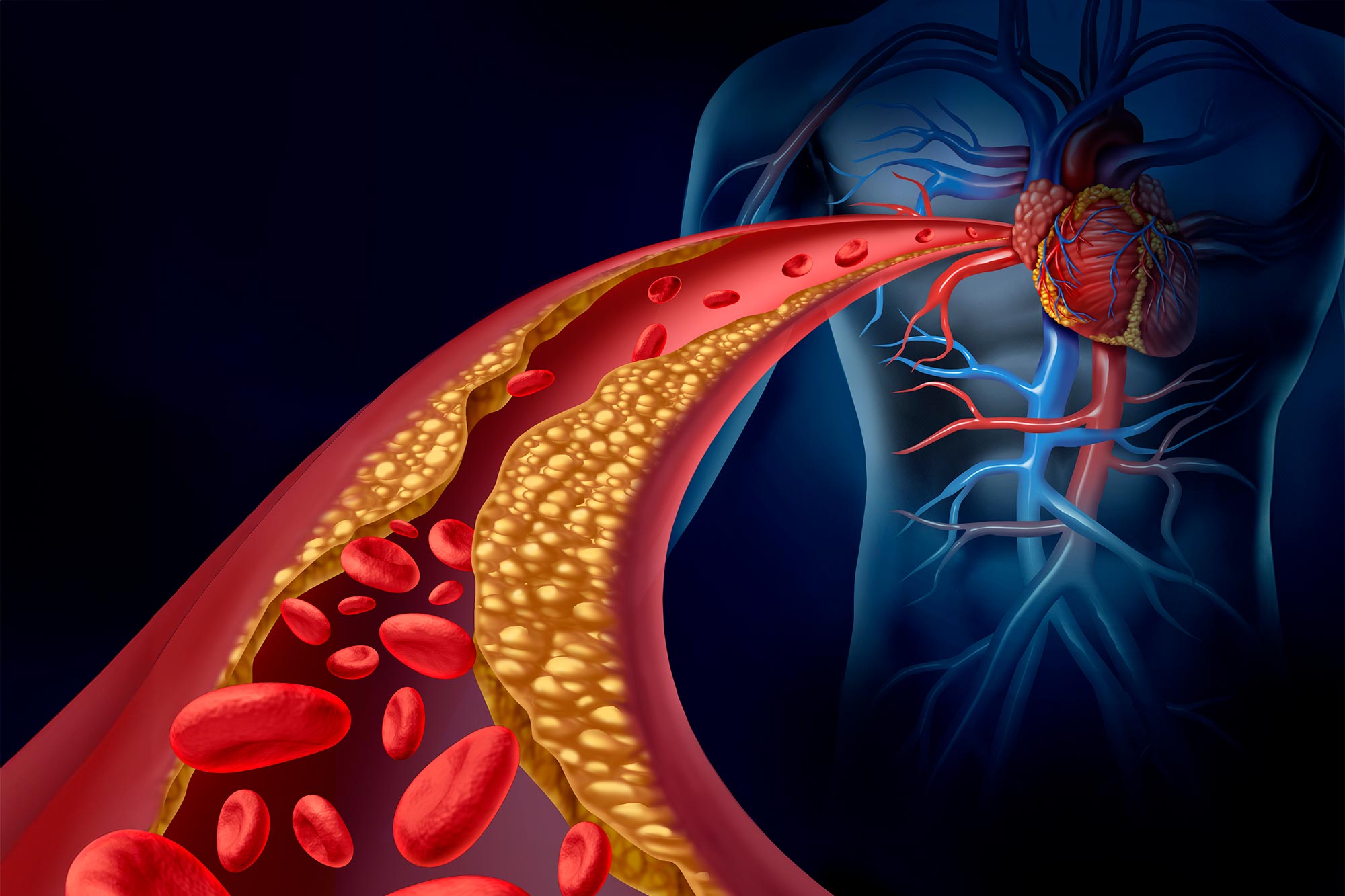
Understanding Atherosclerosis and Its Causes
Atherosclerosis is a condition in which the arteries become narrowed and hardened due to a buildup of plaque. This can restrict blood flow and cause clots to form. It’s an underlying cause of heart attacks, strokes, and peripheral artery disease (PAD), the most common forms of cardiovascular disease (CVD). Atherosclerosis causes coronary artery calcium (CAC), which can be measured non-invasively to predict future cardiac events.
“This groundbreaking study underscores the critical associations of metal exposure from environmental pollution to cardiovascular health,” said Harlan M. Krumholz, the Harold H. Hines, Jr. Professor at Yale and Editor-in-Chief of JACC. “It challenges us to broaden our approach to CVD prevention beyond traditional risk factors and to advocate for stronger environmental regulations, and it underscores the need for continued research in this critical area.”
Research Findings on Metals and Coronary Artery Calcification
Exposure to environmental pollutants like metals is a newly recognized risk factor for CVD, but there isn’t a lot of research on its association with CAC. Researchers in this study sought to determine how urinary metal levels, biomarkers of metal exposure, and internal doses of metals impact CAC.
Researchers used data from the Multi-Ethnic Study of Atherosclerosis (MESA) prospective cohort, tracking 6,418 men and women aged 45-84 from diverse racial backgrounds free from clinical CVD, to measure urinary metal levels at the beginning of the study in 2000-2002. They examined non-essential (cadmium, tungsten, uranium) and essential (cobalt, copper, zinc) metals, both common in U.S. populations and associated with CVD. Widespread cadmium, tungsten, uranium, cobalt, copper, and zinc pollution occurs from agricultural and industrial uses such as fertilizers, batteries, oil production, welding, mining, and nuclear energy production. Tobacco smoke is the main source of cadmium exposure.
Results provided evidence that metal exposure may be associated with atherosclerosis over 10 years by increasing coronary calcification.
Comparing the highest to lowest quartile of urinary cadmium, CAC levels were 51% higher at baseline and 75% higher over the 10-year period. For urinary tungsten, uranium, and cobalt, the corresponding CAC levels over the 10-year period were 45%, 39%, and 47% higher, respectively. For copper and zinc, the corresponding estimates dropped from 55% to 33% and from 85% to 57%, respectively, after adjustment for clinical factors.
Impact and Implications for Future Research
Non-essential and essential urinary metal levels also varied by demographic characteristics. Higher urinary metal levels were seen in older participants, Chinese participants and those with less education. Participants from Los Angeles had markedly higher urinary tungsten and uranium levels, and somewhat higher cadmium, cobalt, and copper levels.
The study’s analysis also considered traditional CVD risk factors such as smoking, diabetes, and LDL-cholesterol levels. The associations between metals and CAC progression were comparable in magnitude to those for traditional risk factors.
“Pollution is the greatest environmental risk to cardiovascular health,” McGraw said. “Given the widespread occurrence of these metals due to industrial and agricultural activities, this study calls for heightened awareness and regulatory measures to limit exposure and protect cardiovascular health.”
Limitations of the study include the unavailability of plaque transition measures in MESA, changes in exposure sources and other factors causing variability of certain measured metals, and the potential for residual and unknown confounding of time-varying exposure measurements.
In an accompanying editorial comment, Sadeer Al-Kindi, MD, Associate Director of Cardiovascular Prevention and Wellness at the Houston Methodist DeBakey Heart and Vascular Center, said the evidence of the study has important implications for public health, health equity and clinical practice.
“The field of environmental cardiovascular medicine, exemplified by this research, offers an emerging frontier in cardiovascular disease prevention and treatment,” Al-Kindi said. “Addressing environmental risk factors like metal exposure will significantly reduce the global burden of cardiovascular disease and address long-standing health disparities.”
Reference: “Urinary Metal Levels and Coronary Artery Calcification” by Katlyn E. McGraw, Kathrin Schilling, Ronald A. Glabonjat, Marta Galvez-Fernandez, Arce Domingo-Relloso, Irene Martinez-Morata, Miranda R. Jones, Anne Nigra, Wendy S. Post, Joel Kaufman, Maria Tellez-Plaza, Linda Valeri, Elizabeth R. Brown, Richard A. Kronmal, R. Graham Barr, Steven Shea, Ana Navas-Acien and Tiffany R. Sanchez, 18 September 2024, Journal of the American College of Cardiology.
DOI: 10.1016/j.jacc.2024.07.020
Never miss a breakthrough: Join the SciTechDaily newsletter.
Follow us on Google and Google News.
1 Comment
“Pollution is the greatest environmental risk to cardiovascular health,” McGraw said. “Given the widespread occurrence of these metals due to industrial and agricultural activities, this study calls for heightened awareness and regulatory measures to limit exposure and protect cardiovascular health.”
As a now eighty year old adult lifetime non-smoking male raised in a smoking household and exposed to secondhand smoke on the job and in public places until those were banned, who’s been addressing mostly mild (now) externally imposed chronic illness for forty-three years and counting, I don’t like throwing a monkywrench into the gears of their research but that quoted statement above is pure nonsense.
Sadly, their formal educations must have never included a (my) kind of nearly subclinical non-IgE-mediated food (minimally) allergy reactions identified, studied and reported on by Dr. Arthur F. Coca by1935 (“The Pulse Test,” 1956), FDA approved food poisoning since the late 1960s and/or excessive related/resultant medical errors; “confounders.” Even while living and working in the L.A., CA, area for almost two decades (1970-1988) I never became as ill from air pollution or tobacco smoke as I have from FDA approved artificially cultured “free” (can cross the blood brain barrier) monosodium glutamate MSG). And, not learning of the true toxicity of or to avoid added MSG until the summer of 2000, I was first diagnosed with high blood pressure, cholesterol and triglycerides in 1992 at forty-eight years of age, after partially avoiding animal fats for a decade for protein allergy reasons. Most, if not all, cohort studies (e.g., 2000-2002) are questionable at best and/or invalid at worst. So, just how common is my kind of tobacco allergy?