
Recent advancements in brain surgery have mitigated the taboo surrounding psychiatric brain surgery, with deep brain stimulation showing promise in treating refractory OCD.
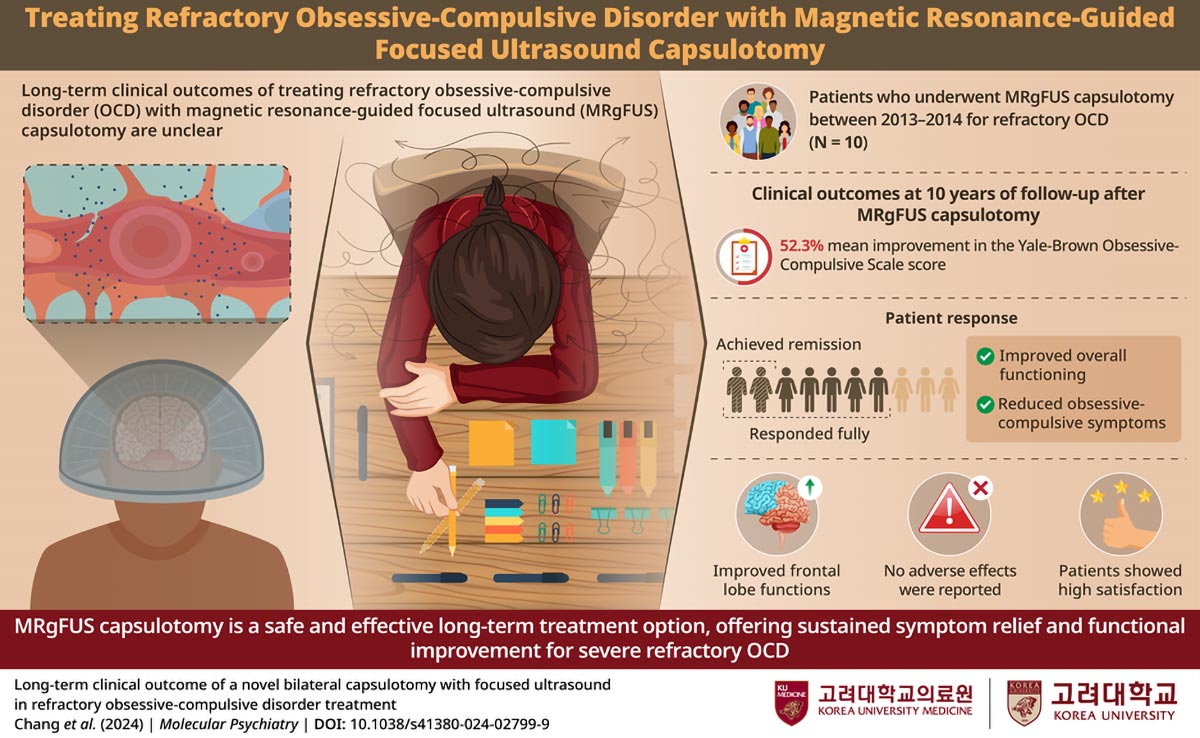
Obsessive-compulsive disorder (OCD) can be highly resistant to standard treatments, profoundly affecting patients’ quality of life. In a groundbreaking clinical trial, researchers tested magnetic resonance-guided focused ultrasound (MRgFUS) capsulotomy as a treatment for severe, treatment-resistant OCD. A 10-year follow-up study revealed lasting improvements in symptoms, enhanced daily functioning, and high levels of patient satisfaction. These findings confirm MRgFUS capsulotomy as a safe and effective option, providing new hope for patients around the world.
Psychiatric Brain Surgery
When conventional non-invasive treatments for psychiatric disorders fail, brain surgery may become a necessary option for clinicians. Historically, this approach has carried a significant stigma, largely due to the notorious history of lobotomies. However, modern advancements in brain surgery are helping to reshape public perception and open new possibilities for treatment.
Breakthroughs in OCD Treatment
One such innovation is bilateral capsulotomy, a procedure often associated with deep brain stimulation. This technique has gained attention for its potential to treat severe, treatment-resistant obsessive-compulsive disorder (OCD). Patients with refractory OCD often struggle with overwhelming, uncontrollable repetitive thoughts and behaviors that severely impair their quality of life, making effective treatment options crucial.
Long-Term Efficacy of MRgFUS Capsulotomy
A group of researchers from South Korea demonstrated that a novel non-invasive bilateral capsulotomy called magnetic resonance-guided focused ultrasound (MRgFUS) capsulotomy is efficacious and safe in treating refractory OCD for up to two years. MRgFUS capsulotomy non-invasively and precisely ablates tissues in the brain region of interest. However, the sustained efficacy of this treatment option was unclear.
Sustained Positive Outcomes
Recently, the same research group conducted a long-term follow-up study of 10 years involving patients with refractory OCD who underwent MRgFUS capsulotomy. They reported that MRgFUS capsulotomy is an efficacious and safe treatment option for refractory OCD, with high patient satisfaction, even at 10 years, establishing its lasting positive effects in patients. Their findings were published in recently in the journal Molecular Psychiatry.
Expanding Applications and Future Directions
This study has achieved multiple milestones in OCD research, offering hope to many patients experiencing refractory OCD. Accordingly, Dr. Jin Woo Chang from Korea University Anam Hospital who is a lead researcher in the study, exclaims, “These studies involve the world’s first clinical trial for OCD with MRgFUS. The current study is also the world’s first long-term follow-up study for OCD after treatment.”
Implications Beyond OCD
Interestingly, the application of MRgFUS capsulotomy may not be just limited to refractory OCD. Dr. Chang says, “The results from our clinical trial also imply the potential role of MRgFUS in managing other common psychiatric diseases, such as refractory depression, due to its simplicity and safety.”
With the clinical application of MRgFUS capsulotomy on the horizon, Dr. Chang concludes, “With the rapid development of new surgical techniques like MRgFUS, it is possible to cure psychiatric diseases without additional complications. I am convinced this new technology will offer a new lease of life for those suffering and struggling from serious psychiatric problems.”
Reference: “Long-term clinical outcome of a novel bilateral capsulotomy with focused ultrasound in refractory obsessive-compulsive disorder treatment” by Kyung Won Chang, Jhin Goo Chang, Hyun Ho Jung, Chan-Hyung Kim, Jin Woo Chang and Se Joo Kim, 28 October 2024, Molecular Psychiatry.
DOI: 10.1038/s41380-024-02799-9
Never miss a breakthrough: Join the SciTechDaily newsletter.
Follow us on Google and Google News.
3 Comments
As someone who’s a long-term sufferer from OCD, I would be curious about any novel approach, but ever since COVID vaccines I’m balking when anyone says “safe and effective”. Particularly when the article implies that this capsulotomy is not neccessarily either of those.
And I’ve obviously read a lot of literature on the disorder over the years, but this is the first time that I’m encountering the term “refractory” OCD, which is curious, so I immediately checked it up elsewhere. And, sure enough, the definition from the article doesn’t match what sparse definitions are found elsewhere. So, “refractory” is not neccesserily “a thing”. What are these people selling?
NIH had a $48 billion 1 year, 2025 budget amd yet had ZERO clinical trials on treating the upstream causes of brain disorders. Why? NIH does not do clinical trials. Drug companies/for profirs do and only IF profitable.
NIH funds tens of thousands of expert researchers with some groundbreakibg results yet then NOTHING happens for cures. NIH has no system to coordinate follow up and no decentralized trials. We need t9 change this. Decentralize trials to be led by clinicians on what works in research and functional medicine.. Drug companies can bid to supply a drug if needed, not lead the trial. Then low cost effective treatments and cures will get to patients.
One example: Lithium orotate a nutrient at .001 dose of Px lithium catbonate works better at reversing memory loss than any Alz drug per Harvard Yankners 8-year trial at a cost of $200/yr vs $22,000/yr. It was on mice, c9nfirmed on human Alz brains. So why 8 years while ZERO patients benefitted. Lithium.orotate has. been used safely for decades in functional medicine and why not treat as Alz is deadly. They die waiting then their brains are used. Yet no clinical trials are likely as drug company do tjhetrials and are making billions on Alz drugs.
NIH meeds to have a Standard of Care and Ethics to REQUIRE >50% of funding be patient-centered focus and a priority to brain disorders. Publish budgrts and have patient advocates on the oversight committees.
NIH had a $48 billion 1 year, 2025 budget amd yet had ZERO clinical trials on treating the upstream causes of brain disorders. Why? NIH does not do clinical trials. Drug companies/for profirs do and only IF profitable.
NIH funds tens of thousands of expert researchers with some groundbreakibg results yet then NOTHING happens for cures. NIH has no system to coordinate follow up and no decentralized trials. We need t9 change this. Decentralize trials to be led by clinicians on what works in research and functional medicine.. Drug companies can bid to supply a drug if needed, not lead the trial. Then low cost effective treatments and cures will get to patients.
One example: Lithium orotate a nutrient at .001 dose of Px lithium catbonate works better at reversing memory loss than any Alz drug per Harvard Yankners 8-year trial at a cost of $200/yr vs $22,000/yr. It was on mice, c9nfirmed on human Alz brains. So why 8 years while ZERO patients benefitted. Lithium.orotate has. been used safely for decades in functional medicine and why not treat as Alz is deadly. They die waiting then their brains are used. Yet no clinical trials are likely as drug company do tjhetrials and are making billions on Alz drugs.
NIH needs to have a Standard of Care and Ethics to REQUIRE >50% of funding be patient-centered focus and a priority to brain disorders. Publish budgrts and have patient advocates on the oversight committees.